


1INSERM, Cochin Institute U1016-CNRS UMR8104, Sorbonne Paris Descartes University, 2APHP Hospital Group Paris Centre Cochin-Hôtel Dieu-Broca, Department of Dermato-venerology, CNR des IST bactériennes-syphilis, 3Sorbonne University, UPMC Univ Paris 06, INSERM, Pierre Louis Insitute of Epidemiology and de Public Health (IPLESP UMRS 1136), Department of Virology, APHP Hôpital Pitié-Salpêtrière, 4AP-HP, Hospital Group Saint-Louis, Lariboisière, Fernand-Widal, CeGIDD, Paris, 5CeGIDD La Joliette-CD13, 6CeGIDD Saint Adrien-CD13, Marseille, 7CeGIDD Aix-en-Provence-CD13, Aix-en-Provence, 8Department of Dermatology, Bel-Air Hospital, CHR Metz-Thionville, Metz, 9CeGIDD of Nancy, Nancy, 10Department of Dermatology, Jean Bernard Hospital, Valenciennes, and 11AP-HP, Hospital Group Paris Centre Cochin-Hôtel Dieu-Broca, Department of Bacteriology-CNR Streptocoques
Benzathine penicillin G (BPG) is the reference treatment for early syphilis, but shortages have recently been reported, highlighting a need for the validation of alternative treatments. The aim of this study was to evaluate the genomic resistance of Treponema pallidum subspecies pallidum (TPA) to macrolides and doxycycline in France. Swabs from genital, anal, oral and cutaneous lesions were obtained from 146 patients with early syphilis in France. They were screened for mutations conferring resistance to macrolides and doxycycline by nested PCR and sequencing. Resistance to macrolides was detected in 85% of the isolates, but no point mutations conferring doxycycline resistance were detected. These findings confirm that, in France, resistance to macrolides is widespread. Moreover, we confirmed the absence of genomic resistance to doxycycline in the TPA strains. Therefore, doxycycline could be safely recommended as an alternative to BPG for the treatment of early syphilis.
Key words: syphilis; Treponema pallidum subs pallidum; antibiotic resistance; doxycycline; macrolide.
Accepted Jun 25, 2020; Epub ahed of print Jul 3, 2020
Acta Derm Venereol 2020; 100: adv00221.
Corr: Nicolas Dupin, Hôpital Cochin – Pavillon Tarnier, U1016, Equipe Biologie Cutanée – CNR IST bactériennes – Syphilis, 89, rue d’Assas, FR-75006 Paris, France. E-mail: nicolas.dupin@aphp.fr
Benzathine penicillin G is the reference treatment for early syphilis, but shortages have been reported recently, highlighting a need for the validation of alternative treatments. The aim of this study was to evaluate the genomic resistance of Treponema pallidum subspecies pallidum to macrolides and doxycycline in France. Swabs from mucosal and cutaneous lesions were obtained from 146 patients with early syphilis. Resistance to macrolides was detected in 85% of the isolates, but no mutations conferring doxycycline resistance were detected. These findings confirm that resistance to macrolides is widespread and no evidence for genomic resistance to doxycycline was detected.
Syphilis is a sexually transmitted infection (STI) that remains a public health problem throughout the world. There are an estimated 18 million cases of syphilis worldwide, with a global incidence of 6 million new cases every year (1). According to the latest data from the European Center for Disease Control and Prevention (ECDC), syphilis rates in Europe reached 7.1 cases per 100,000 inhabitants in 2017 (2). The European nations with the highest rates of syphilis were Iceland, Malta, the UK and Spain (more than 9 cases per 100,000 inhabitants) (2). The real incidence of syphilis in France is difficult to determine, but the number of cases recorded by the RésIST network (a French network of clinicians reporting clinically diagnosed syphilis and gonorrhoea) is stable and estimated at approximately 1,500 cases per year (3).
The advent of antiretroviral therapy for HIV infections led to a resurgence of syphilis, with case numbers increasing since 1999–2000, due, at least partly, to a decrease in prevention and safe sexual practices (4–6). Epidemiological studies have shown, as in most Western countries, that syphilis in France essentially affects men who have sex with men (MSM) (3), with a prevalence of 79% in 2018. Moreover, and although this is controversial, with the development of pre-exposure prophylaxis (PrEP) to prevent HIV transmission (7), increases have been reported in the number of cases of syphilis, gonorrhoea and chlamydial infections (8, 9), maybe because of the screening for STIs being treated as more important in this population.
American (Centers for Disease Control and Prevention 2015) (10) and European guidelines (2014) (11) currently recommend benzathine penicillin G (BPG) for the treatment of early and non-neurological late syphilis. Several alternative antimicrobial treatments have also been proposed, including macrolides and tetracyclines. An African study showed that two 1 g doses of azithromycin, administered on the same day, were as efficient as a single dose of BPG for the treatment of early syphilis (12). However, mutations at positions A2058G and A2059G in the 23S rRNA gene of Treponema pallidum subspecies pallidum (TPA) have been reported to confer clinical resistance to azithromycin (13). The A2059G mutation seems to be infrequent in North America, Europe and Asia, whereas the A2058G mutation appears to be widespread in these areas (14, 15). Azithromycin cannot, therefore, be recommended as an alternative to BPG in these countries.
Tetracycline is a broad-spectrum antibiotic of choice against bacterial STIs. Resistance to tetracycline is conferred by mutations of the 16S rRNA gene affecting positions 965–967 (AGA965-967TTC) in Helicobacter pylori (16), 1058 (G1058C) in Propionibacterium spp. (17) 926–928 (AGA926-928GGA, AGC, TTC) and 939 (A939C) in Helicobacter pylori (18, 19). These mutations induce a change in the conformation of the binding site for tetracyclines that is associated with resistance. Several studies have reported an absence of point mutations in the 16S rRNA gene of TPA DNA in samples from Asia (20, 21). In Europe, surveillance for doxycycline resistance has been evaluated only in Italy and Spain in, respectively, 53 cases and 62 cases, and no point mutations were detected in these genes in these countries either (22, 23).
In France, the use of doxycycline to treat syphilis increased between 2013 and 2017, due to a disruption of the supply chain for BPG (24–26). The development of PrEP to prevent HIV transmission also led to an increase in the number of new cases of bacterial STIs, including syphilis (8, 9). However, doxycycline has been shown to decrease the incidence of chlamydial infections and, to a lesser extent, syphilis, when used for post-exposure prevention (PeP) (27). It is therefore critically important to investigate the possible existence of molecular mechanisms that could lead to the development of doxycycline resistance in TPA strains circulating in France and, more generally, in western countries, as this aspect has been explored only in Asia and a limited number of countries in Europe.
This study evaluated the rate of resistance to macrolides and doxycycline in TPA strains from patients with syphilis in France.
Sample collection
Swabs from genital, oral, anal and cutaneous lesions were collected anonymously from patients with primary and secondary syphilis attending STI centres in Paris (n = 97; 66%), Marseille (n = 30; 20.5%), Aix-en-Provence (n = 8; 5.5%), Thionville (n = 7; 4.8%), Nancy (n = 3; 2%) and Valenciennes (n = 1; 0.7%), between October 2010 and January 2017. Clinical data, including patient’s age, sex, sexual orientation and HIV status were also collected. The lesions sampled for this analysis were collected from the following sites: genital (n = 95), anal (n = 24), buccal (n = 19) and cutaneous (n = 8). Qualified staff collected the samples by squeezing the lesion area gently and imbibing the swabs with the exudate. The swabs were then placed in sterile tubes containing 1 ml phosphate-buffered saline (PBS) (150 mM sodium phosphate, 150 mM sodium chloride) for DNA extraction. Samples were frozen at –80°C until their use for DNA extraction. Sample collection was authorized by the Human Subject Committee of each of the participating institutions (GENOSYPH protocol, CPP no. SC3005) and informed consent was obtained from each patient. Anonymized specimens were then sent to the National Reference Center for STIs with expertise in syphilis, at Cochin Hospital in Paris. PCR was performed, to check for the presence for TPA DNA by amplifying a specific fragment of the TPA tpp47 gene, as described by Grange et al. (28). All the samples analysed in this study tested positive for TPA DNA.
Syphilis diagnosis
The diagnosis of clinically active early syphilis (primary or secondary) was based on Centers for Disease Control and Prevention criteria (CDC 2015) (10) and the 2014 European guidelines (11). All patients classified as having probable or confirmed syphilis were considered to have syphilis for the purposes of this study.
DNA extraction
DNA was extracted from 200 ml of swab exudate with the NucleoSpin® Blood (Macherey-Nagel Eurl, Hoerd, France) kit, according to the manufacturer’s instructions. We used 200 µl of sample combined with an equal volume of lysis buffer containing guanidine hydrochloride, Tween 20 and 1.4 mg/ml proteinase K, incubated for 30 min at 70°C to achieve lysis. DNA samples were stored at 4°C for no more than 2 days before testing, thereby avoiding the need for repeated freeze/thaw cycles. For long-term storage, samples were frozen and stored at –20°C.
Detection of genetic resistance to macrolides and doxycycline
DNA samples were screened for macrolide resistance (mutations at positions 2058 and 2059 of the 23S rRNA gene) (29) and tetracycline resistance (mutations at positions 965–967, 926–928, 939 and 1058 of 16S rRNA gene) (16–19) by nested PCR and sequencing. A DNA sample from the TPA strain Nichols (5 pg/μl) was used as a positive control.
For the 23S rRNA gene, nested PCR was performed as described by Grillová et al. (29). The PCR mixture in the first step contained 2 μl of a 2.5 mM deoxynucleotide triphosphate (dNTP) mixture, 5 μl of 5× PS GXL buffer, 1 μl of each primer (10 pmol/μl), 0.1 μl of PrimeSTAR GXL polymerase (Takara Bio Europe, France), and 1 μl of DNA, with PCR-grade water added to a final volume of 25 μl. The 23S rRNA gene was amplified by PCR under the following conditions: 94°C (1 min); 98°C (10 s), 68°C (15 s) touchdown (–1.0°C per cycle), and 68°C (1 min 45 s) for 8 cycles; 98°C (10 s), 61°C (15 s), and 68°C (1 min 45 s) for 35 cycles, with final extension at 68°C (7 min). In step 2, the PCR mixture contained 0.5 μl of 10 mM deoxynucleotide triphosphate (dNTP) mixture, 2.5 μl of ThermoPol reaction buffer, 0.25 μl of each primer (100 pmol/μl), 0.05 μl of Taq polymerase (5,000 U/ml; New England Biolabs, Ipswich, MA, USA), and 1 μl of the product of the PCR performed in the first step. PCR-grade water was added to a final volume of 25 μl. The second PCR amplification was performed under the following cycling conditions: 94°C (1 min); 94°C (30 s), 48°C (30 s), and 72°C (1 min, 15 s) for 40 cycles; with a final extension at 72°C (7 min). For the 16S rRNA gene, nested PCR was performed as described by Wu et al. (21). In the first step, PCR was performed in a final volume of 25 μl, to amplify a 748 bp fragment. Each reaction mixture contained 0.5 μl of 1 mM deoxynucleoside triphosphates (dNTPs), 2 μl of each primer at a concentration of 10 pmol/l (16S rRNA out-F 5’-GTGGATGAGGAAGGTCGAAA-3’ and 16S rRNA out-R 5’-CAGAGTCCCCAACACCACTT-3’), 0.3 μl of a 1 U/μl preparation of high-fidelity Taq polymerase (Platinum Pfx DNA polymerase, Thermo Fisher Scientific), 2.5 μl of 10× PCR buffer, 1.5 μl of MgCl2 and 10 μl of template DNA. PCR-grade water was added to a final volume of 25 μl. The second-step PCR was performed in a final volume of 25 μl containing a 3 μl aliquot of the product of the first round of PCR, to amplify a 531 bp fragment. The composition of the reaction mixture was identical to that for the first PCR, except for the amount of MgCl2 solution added (0.5 μl) and the primers used: 16 rRNA inner-F (5’-TCAACTTGGGAACTGCACTG-3’) and 16S rRNA out-R. PCR-grade water was added to a final volume of 25 μl. The amplification conditions for both PCR assays were 94°C for 5 min, 20 cycles for the first step and 40 cycles for the second step as follows: 94°C for 1 min, 68°C for 1 min and 72°C for 1 min, and a final extension at 72°C for 10 min. The amplicons were then checked by subjected a tenth of the total volume of the amplification reaction to agarose gel electrophoresis in a 1% agarose gel in the presence of ethidium bromide, with visualization of the bands obtained under UV light. For sequencing, PCR products (the remaining nine-tenths of the total reaction volume) were cleaned up by ultrafiltration under a vacuum with the NucleoFast 96 PCR kit (Macherey & Nagel). DNA concentration ranged from 8 to 36 ng/µl, based on the absorbance values obtained at 260 nm. Amplicons were sequenced by the Sanger method with the ABI PRISM BigDye V3.1 Terminator kit (Applied Biosystems), according to the manufacturer’s instructions, and were analysed on an ABI PRISM 3100 DNA sequencer (Applied Biosystems). DNA sequences were analysed with ALIVIEW Software.
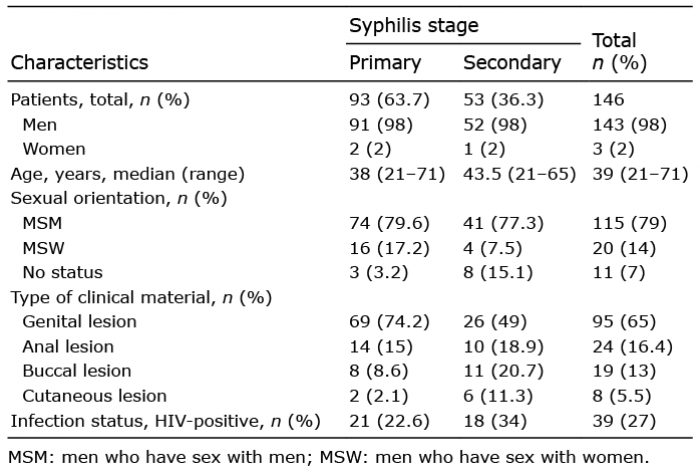
In total, 146 samples were collected from 146 patients (1 sample per patient) from October 2010 to January 2017, from patients with early syphilis attending STI centres or hospitals at several sites in France. most of the patients were male (80%). They were aged between 21 and 71 years and 33% had HIV infection. Most of the patients were MSM (80%). The swabs were collected from the genital area for 95 patients (65%), the anal area (n = 24, 16.4%), the mouth (n = 19, 13%) or the skin (n = 8, 5.5%). According to the CDC criteria, 93 patients were diagnosed with primary syphilis (63.7%) and 53 patients (36.3%) were considered to have secondary syphilis (36.3%) (Table I). All samples tested positive for TPA DNA in routine PCR analysis (tpp47); the 23S and 16S rRNA genes were then amplified from each sample, as genetic markers for resistance to erythromycin and doxycycline, respectively. Amplification efficiency was 89% (n = 130) for the 16S rRNA gene, and it was possible to sequence 127 of the amplicons obtained (98%). The amplification efficiency for the 23S rRNA was lower, at 71% (n = 104), but it was possible to sequence all the amplicons obtained (100%).
No mutation of the 16S rRNA gene was detected in any of the samples analysed. A large proportion of samples presented genetic resistance to macrolides, with the A2058G mutation of the 23S rRNA gene present in 85% of the population tested (n = 88). We found no difference between the primary and secondary stages of syphilis (Table II). None of the samples presented the A2059G mutation.
Table I. Clinical characteristics of the patient population
Table II. Analysis of genetic resistance to macrolides and doxycycline in the population
The first-line treatment for early syphilis is BPG (10, 11), with no rival treatment of equivalent efficacy. The only alternative currently available is a 2-week course of doxycycline. Macrolides, such as azithromycin, are not recommended in European countries, Australia or China (30), due to the high rates of resistance to these drugs in TPA strains. In the USA, azithromycin is still listed as an alternative when treatment with penicillin and doxycycline is not feasible; meanwhile, the high rate of resistance to macrolide in this country (31). In this context, the primary goal of this study was to assess the frequencies of the A2058G and A2059G mutations of the 23S rRNA gene responsible for macrolide resistance in the DNA of the TPA strains from patients. As expected, macrolide frequency was high, at 85% in clinical isolates from various regions of France. This result is consistent with the findings of a previous study reporting a resistance rate of 86.4% in the population studied (32). Macrolide resistance has been emerging in TPA over a period of more than 20 years, and this resistance is now widespread. The spread of macrolide resistance may be due, at least in part, to the frequent use of antibiotics of this class, and of azithromycin in particular, to treat other STIs, such as Chlamydia trachomatis and Mycoplasma genitalium urethritis and cervicitis (33). The recent emergence of azithromycin resistance in Mycoplasma genitalium has been attributed to an increase in the use of this antibiotic to treat chlamydial infections (34) and has led to the establishment of new recommendations favouring doxycycline (200 mg per day for 7 days) as the first-line treatment of uncomplicated chlamydial infection (35).
The presence of mutations of the 16S rRNA gene or the acquisition of genes capable of decreasing susceptibility to doxycycline (36) has never been investigated in a population of French patients with syphilis. We addressed this issue by analysing point mutations in the 16S rRNA gene of TPA DNA, known to induce doxycycline resistance when they occur in the equivalent genes of other bacteria. We found no such mutations in any of the samples studied. This finding is consistent with those of previous studies on syphilis patients in China and Southern Europe exploring point mutations at positions 965–968 and 1058 of the 16S rRNA gene (20, 22, 23). We also explored 2 other previously described point mutations (21), at positions 927–928 and 939 of the 16S rRNA gene, neither of which was found in any of our patients. In our cohort, we do not have information about the number of patients receiving doxycycline treatment. However, in a previous prevalence study conducted by the National Reference Center in Paris, we have shown that approximately 5% of patients had been treated by doxycycline for early syphilis between 2000 and 2007 (37).
Resistance can also be linked to the presence of tet genes in bacterial genomes (38) where the tet(M) gene plays a major role in tetracyclines resistance in genital bacteria, including Mycoplasma spp and Ureaplasma, (39). To date, whole-genome sequencing of TPA strains did not demonstrate the presence of tet genes. Therefore, searching for such gene in our study did not seem relevant.
The lack of evidence for genomic resistance to doxycycline in TPA suggests that this antibiotic can safely be used to treat early syphilis and for post-exposure prophylaxis against infections caused by TPA strains in populations of MSM exposed to PrEP. However, continuous monitoring is required to detect the possible occurrence of doxycycline-related mutations in this population.
In conclusion, resistance to macrolides was widespread, but no genomic resistance to doxycycline was detected in this study.
This work was supported by grants from the “Association de Recherche en Virologie et Dermatologie (ARVD)” and the French Society for Dermatology (SFD).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize